
DCA blog by Jie Gao, PhD candidate in Department of Human Geography and Spatial Planning at Utrecht University. Based on an article written together with Marco Helbich, Martin Dijst, and Carlijn B.M. Kamphuis. For the full article with all references and details, please follow this link.
The Netherlands is well known for the prevalence of walking and cycling for transportation purposes. Cycling accounts for approximately a quarter of all journeys and about one-tenth of all kilometers traveled. Nevertheless, there is room for improvement, since about 30% of the commuting trips within five kilometers are still made by car. The World Health Organization (WHO) recommends more active travel (i.e., walking and cycling) in people’s daily life to reduce the risk of non-communicable diseases. Therefore, policy-makers are advised to develop strategies that stimulate active travel and discourage motorized transport.
To make the health benefits of walking and cycling more apparent to policy-makers, we combined cycling statistics with the World Health Organization’s (WHO) new computational tool for the study. The Health Economic Assessment Tool (HEAT) provides a method to estimate the number of deaths prevented by the beneficial health effects of both walking and cycling.
In a country like the Netherlands, where walking and cycling levels are high, differences in walking and cycling between population groups may be presumed to be considerable, which could significantly contribute to health inequalities in the population at large. We used the data collected on the average amount of time spent per person per week (in minutes) on walking and cycling by different population groups.
Just one example is how differences in walking and cycling translate into differences in health benefits in the Netherlands. A study on the active travel and health benefits from Gao et al. (2017).
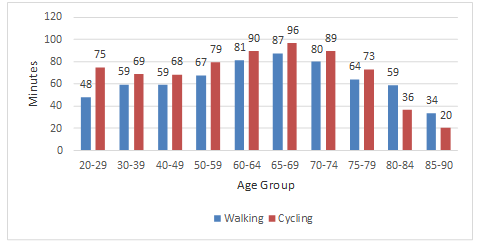
Walking and cycling levels of different age population groups
In general, Dutch adults spent 63 minutes on walking and 75 minutes on cycling per week. The duration of both activities peaks at around 65-69 years and starts to decline at the age of 80 (Figure 1). Cycling duration per week for men and women was nearly equal (75 versus 74 minutes). In contrast, women walked more (70 minutes) than men (57 minutes).
Health benefits of walking and cycling for different age population groups
The number of deaths prevented by walking and cycling was greatest among the age groups of and 80-84 and 75-79 years, respectively (Figure 2). Despite the small population size of these elderly compared to younger people, death prevention was much higher among the elderly because of their relatively high levels of walking and cycling and their higher mortality rate. The reduction in mortality rate was a direct result of the average walking and cycling duration for the target group.
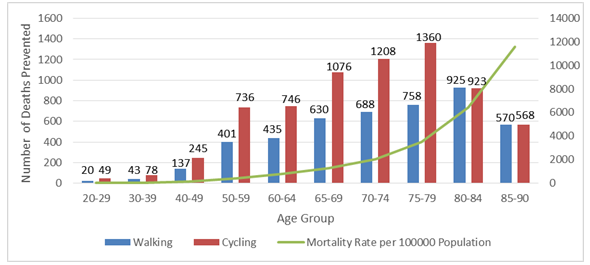
We found that people in their early stage of retirement (age 65-75) walked and cycled more than members of other age groups. More free time combined with relatively good health may offer them the opportunity to spend more time on active travel.
Conclusion
This study used HEAT to estimate the mortality rate reduction (i.e. a direct result of average walking and/or cycling durations) and the number of deaths prevented by walking and cycling at a population level (i.e. taking the size of the population subgroup and the average mortality rate into account). Our findings suggest that a large number of prevented deaths in some population subgroups does not always reflect high walking and cycling levels, but can also stem from a large population size, a high mortality rate or both. Particularly among senior citizens, as a result of their relatively high mortality rates and high walking and cycling levels, a large number of deaths were prevented.
Results show that more attention should be paid to subgroups with a high mortality rate and large population size but low walking and/or cycling levels, which are for instance the lower socioeconomic groups. Urban planners and policy makers should develop strategies and interventions to increase walking and cycling levels among lower socioeconomic groups, which finally may reduce socioeconomic inequalities in health.
Reference:
Gao, et al. (2017). Socioeconomic and demographic differences in walking and cycling in the Netherlands: How do these translate into differences in health benefits? Journal of Transport & Health.
You must be logged in to post a comment.